I know it’s been a minute, but I swear I have a good reason–as of this month, I am now in private practice! Unsurprisingly, I’m specializing in grief and trauma. My goal is to have at least a certificate in Thanatology by the end of the year.
I want to also say that I have loved my 3+ years at various mental health organizations. It provided me with incredible opportunities for professional growth (not to mention, allowing me to put my existential navel-gazing to good use). I realized when I was wrapping up at my previous job just how many different clients I’ve had the pleasure of working with over the years. Each one had a different diagnosis and with each discharge, the breadth of my experience sank in a little bit more.
I’m currently pouring a lot of time into my new self-care project, afternoonified.art, where I draw people who both do and do not exist. I’m really getting into portraits that tell a story without using the face as well.
My internal weather is certainly changing in a positive way, and I hope it’s not too forward to share this leg of my journey with you. After all, we’ve only been together for eight years now. (We have to stop meeting like this; people will talk.)
Until next time, stay sane and safe! Know your worth; then add tax.
I promised we’d take a look at the consequences of long-term stress (and, by association, trauma) on the body, didn’t I? That’s today’s topic so buckle up, Class.
Before I jump in, I want to define a few terms so we’re all speaking the same language.
The amygdala is a little almond-shaped cluster that controls your emotions–namely, fear and the fight/flight/freeze response. Memory and decision-making are also controlled by the amygdala.
The autonomic nervous system controls all unconscious processes, like breathing, blood pressure, and heart rate. Think of it like a car with automatic transmission, or being on autopilot.
Adrenal glands produce adrenaline and cortisol when the body reacts to a stressor. The inner medulla is the part that produces the hormones epinephrine and norepinephrine, which help kick off the whole fight-or-flight response.
In a nutshell:
Stressors trigger the sympathetic nervous system and hormones come rushing in full-bore. The amygdala enters the chat, which sets off a chain reaction with the adrenal glands and other endocrine systems. Your blood pressure goes up, your heart rate increases, you sweat. Without you even noticing it, your body is preparing to take one of three paths: fight, flight, or freeze.
When in crisis, our bodies and minds work in tandem to respond to the situation. The good old autonomic nervous system kicks into gear, triggering an immune response (which is designed to protect the body and fight off “intruders,” so to speak)1. This immune response releases histamines, which are also the cause of hay fever symptoms like itchy eyes and hives. It may sound counterintuitive, but all of these unpleasant symptoms are part of your body’s fight to keep you alive. The second the stress hit that tiny little amygdala, you were no longer in the driver’s seat. Ever since that moment, you’ve been on autopilot–think of your body as a kind of gundam suit designed to protect you by any means necessary. This response is as effortless and natural as breathing.
When most people hear the word “adrenaline,” they often imagine a scene such as a mother lifting a car off her baby. Our entire autonomic nervous system is wired to keep us alive, and the body can do incredible things when under acute stress.
However, you can’t sustain that level of intensity forever. Think of a rubber band. You can only stretch it so much before it begins to lose some of its elasticity, and the same principle applies to stress and the body. Our bodies are not built to sprint at 84,000 miles per hour 24 hours a day, 8 days a week, and that’s precisely what long-term stress demands of you.
Miller, Chen, and Parker (2010) describe stress as something that “accumulates” in the body’s cells. What this means for you, dear Reader, is that your body is in a constant state of inflammation because those hormones are poppin’. Even if it’s more of a wallflower than the life of the party, that inflammation is still there.
This leads us to our next point: vulnerability for chronic illness. When your body is constantly on high-alert, it reacts to stimuli that may not bother the average bear. Many trauma survivors have at least one, if not multiple, chronic health conditions. Autoimmune disorders such as lupus are more common in adult cis female trauma survivors2. Additionally, the odds of an autoimmune disorder causing an individual’s first hospitalization were higher among adults who reported two or three different types of childhood adversity, such as physical, sexual, and/or verbal abuse; parental neglect; or having a parent or caregiver who struggles with substance abuse or mental illness3.
There is a strong behavioral component to this complex issue as well. Early trauma leads to hypervigilance and mistrust, meaning there are cognitive and emotional factors layered on top of the biological aspect. (It’s like the world’s worst sandwich, basically.)
Let’s pause for a visual aid. I wonder how many of you are familiar with our good friend Ouroboros.
Picture the biological factors as the head of the snake, and the cognitive/emotional factors as the tail. Or reverse it. Either way, they are simultaneously feeding and devouring each other. Much like our old pal Anxiety, stress feeds itself.
So, that probably sounds terrifying, right? It doesn’t have to be. Here are some platitudes to explain why:
Knowledge is power.
Know thy enemy.
If it bleeds, we can kill it.
If we know what our own vulnerability factors are, we can find ways to counter them. If you have a chronic illness, make sure you’re keeping in touch with your doctor and taking any medications you’re prescribed. Try to eat well, stay hydrated, get enough sleep. Take at least a minutes throughout the day to do something you enjoy and celebrate being alive. A client once very astutely described living (versus surviving) as “nurturing the being as well as the human.” We exist on many levels–physical, emotional, cognitive, spiritual. Please be kind to yourselves and send love into the darkness.
One final note:
Take care of yourselves, Readers. Go take a safe, socially distant rainbow walk. Get some vitamin D–it’s good for you! Read a book. Plant a tree. Take a hot shower with a frozen orange. Meditate. And for the love of god, wear a mask and stop touching your face.
1 Quas, J. A., Bauer, A., & Boyce, W. T. (2004). Physiological reactivity, social support, and memory in early childhood. Child Development, 75(3), 797-814.
3. Miller, G. E., Chen, E, & Parker, K.J. (2011). Physiological stress in childhood and susceptibility to the chronic diseases of aging: Moving toward a mdoel of behavioral and biological mechanisms. Psychological Bulletin,137(6), 959-997.
I’m finishing up the final installment of the ACEs series, but I realized I haven’t told you about the rainbow walk yet.
I began using this exercise with clients when I was a wee intern–as part of the PRP program, we were required to do a certain number of “off-site” classes, so finding creative ways to get the clients out and about was a challenge. The rainbow walk is a great way to pair mindfulness with physical activity and fresh air, if you’re able and comfortable with going outside. If not, you can also do this from the comfort of your own home.
Essentially, you just…go for a walk. And as you’re walking, you pay attention to your surroundings and name all the red things you see, all the orange things, and so on. It’s kind of like that road trip game where you count all the blue cars, except better because you’re not actually stuck in a car. The point of the exercise is to bring yourself back to the present moment and focus one-mindedly on a task–in this case, using just one sense to observe.
Anyway, just a quick little bonus post so you’re not completely lost when I post ACEs Part 4 tonight. See you then!
Disclaimer: Growing up in the Midwest, I never encountered any actual stories/incidents of cow-tipping. But my god, I wish I had.
In 1959, Carl Rogers coined the acronym “COWs,” or Conditions of Worth. According to the man himself:
“The self-structure is characterized by a condition of worth when a self-experience or set of related self-experiences is either avoided or sought solely because the individual discriminates it as being less or more worthy of self-regard.… A condition of worth arises when the positive regard of a significant other is conditional, when the individual feels that in some respects he is prized and in others not. Gradually this same attitude is assimilated into his own self-regard complex, and he values an experience positively or negatively solely because of these conditions of worth which he has taken over from others, not because the experience enhances or fails to enhance his organism.” *
TL;DR: We crave unconditional positive regard from our caregivers pretty much from the get-go (example: “I will love you no matter what”). Unfortunately, a lot of times, you end up with a child receiving the message (whether overtly or through subtext) “I love you if/when you ___” and/or “You’re bad/undeserving of love/etc. if you [insert thing that caregiver/person of influence has determined is bad].”
That’s radically different than the message of “I love you, you’re safe, I’ll take care of you” that we instinctively need. Again, the pleasure principle applies: We’re hardwired to gravitate toward what feels good and avoid what feels bad.
Ironically, it’s the uncomfortable things that stick in our minds. Think about a time you received a critique at work or got into a fight with a loved one. When you think about that day, what do you remember most–the critique/fight or everything else you did within that 24-hour span?
That negative little voice in your head–whose is it? A parent? A friend? A romantic partner? …
Yourself?
This is where core beliefs come into play, but that is an entirely different discussion for another day. In the meantime, take a look at this worksheet for more info on core beliefs and how to identify yours.
This is one of the reasons why those pesky ACEs are so persistent, even years later. We may be designed to move toward the comfortable, toward stasis, and yet we’re awesome at making ourselves miserable.
The next post in this series will focus on the biology of chronic stress and how ACEs can be a risk factor for certain illnesses. In the meantime, readers, take a moment to reflect on the following questions about your own inner monologue/critic.
* Rogers C (1959) ‘A Theory of Therapy, Personality, and Interpersonal Relationships, As Developed in the Client-Centered Framework’, in Koch S (ed) (1959)
Okay, so now that we know what ACEs are, let’s get a little more personal.
To begin, I’d like to share with you two pictures from my childhood.
1993, age four
1994, age five – kindergarten photo
Are these the same child?
Yes.
In the photo on the left, I am dolled up and mugging for the camera. I’m not sure who took me to get my photo taken that day (probably at Sears). If it was my biological mother, she was having an exceptionally good day. The reality is that one of my aunts probably arranged the whole thing. But I look happy, round-cheeked, grinning at the camera with a twinkle in my eyes.
In the photo on the right, taken roughly a year and change after the first, I am posing for my kindergarten photo. I was grumpy partly because of that damn cowlick, but also because my home life had basically gone to hell in a handbasket in the space of a year. My mother was drinking again, heavily. She would often leave me alone in the house at night to go out to bars. One of my earliest memories is waking up alone and wandering through the darkened house. I walked outside and paced the sidewalks for what felt like hours, watching as the lights in the houses lining the street flickered off, one by one by one.
Readers, that is the loneliest I have ever felt in my life.
If we ignore the backstory and focus only on the images (lighting and photo quality aside), what remains is this: The girl on the right has lost all the baby fat from her cheeks. Her eyes are huge, dark, and sunken. She is trying to smile but her teeth are gritted. She does not look at the camera, but rather past it, as if trying to see something in the distance. You know, that old chestnut–the Thousand Yard Stare. Still a cute kid, but not the type of child you’d look at and go, “Oh, yeah, she’s doing well.”
Chronic stress changes the body in a myriad of different ways. I’ll touch on the biology of chronic stress (behavioral medicine is a fascination of mine) in the next post, but for now, let’s focus on face.
They say the eyes are the windows to the soul. If we peeked through your windows, what might we find? I’m looking forward to hearing from you, readers!
Disclaimer: The information contained in this post is not intended to diagnose or treat any condition. I am a licensed therapist, but I am not your therapist.
I ACEd the quiz! Tongue firmly in cheek, of course. There is no quiz, but today I would like to touch on trauma and its physical effects–hence the reference to ACES, or the Adverse Childhood Experiences Scale.
As any even casual reader of the blog knows, trauma is kind of My Jam. I love working with clients who are struggling with the same core issues I struggled with the first 20+ years of my life. I knew that was going to be bailiwick from the time I started therapy myself, at 18, but I didn’t really do much with it until I entered grad school and suddenly had to write a thousand different papers (that were not centered around arguing whether the box of money in Faulkner’s The Sound and the Fury is actually a box of shit. Look it up. It’ll change your life).
When I got my very first assignment, my brain went “PING!” and told me trauma was the area to hit. It’s a touchy area, for sure. Go too fast, and you risk re-traumatizing your client and damaging rapport. Go too slowly, and your client will stagnate. It’s like a dance.
I’d love to wax poetic about the biology of chronic stress and implications for adulthood, but that needs its own post.
On to the significance of ACEs. The instrument itself is simple–ten self-report items, scored either “0” or “1.” I’ve re-typed it here for the sake of your eyes, but you can see the original and lots of great info on acestoohigh.com.
To avoid inadvertently triggering readers, I’m going to put the actual scale underneath this spoiler tag, as the questions do involve all forms of child abuse.
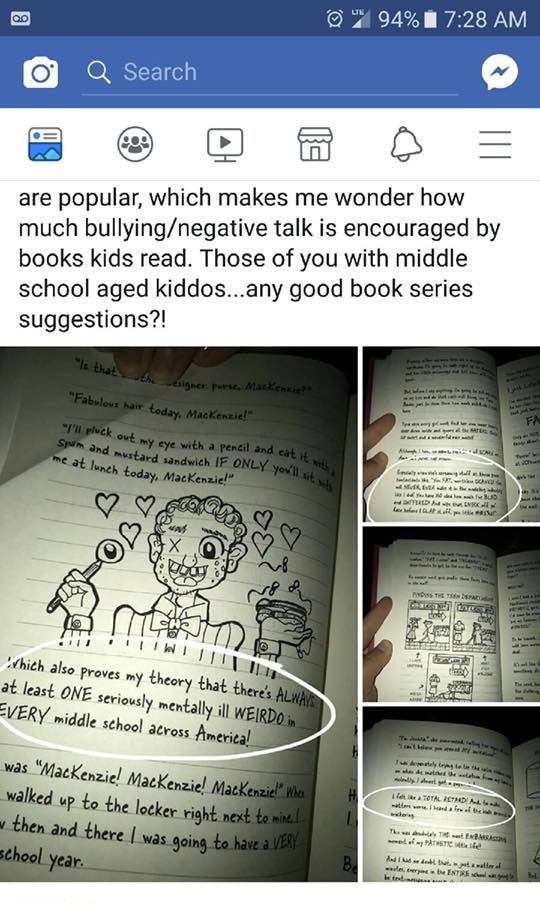
I have not been this angry and unsettled about a piece of pop culture since the Fear VR: 5150 Knotts Berry Farm debacle of September 2016. This afternoon, I happened upon a post made by one of my Facebook friends regarding a book series called “Dork Diaries,” which is aimed at children (particularly girls) aged 8 to 14. The protagonist is a 14-year-old girl named Nikki Maxwell and her life as a middle schooler.
Before I get into the meat-and-potatoes of this post, I want to warn you that the following images contain extremely discriminatory language that some readers may find upsetting. All images were provided via a good friend of mine on Facebook who is also a mental health advocate and fights like hell against the stigma. I respect her deeply and am grateful to her for bringing this to my attention.
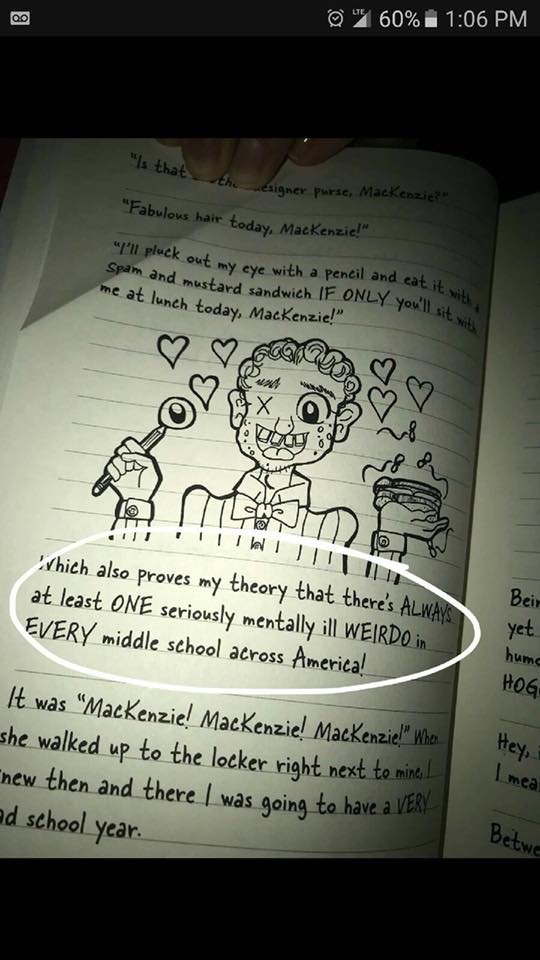
Below is the first image I saw regarding this series.
Let me begin by stating that I have not read any of the books in their entirety and had no idea they even existed until just a few hours ago. I also hate that by writing this post, I am giving this author more attention. However, I cannot let this issue go unaddressed for a number of reasons. For the sake of brevity, I’ve made a list:
Stigmatizing language hurts all of us, and we need to knock it off. Seriously
The age range AND gender at which the books are targeted is highly disturbing, given the nature of the content. I’m not talking about the whole “celebrities being seen without panties but not phones” bit that many reviewers have cited as problematic.
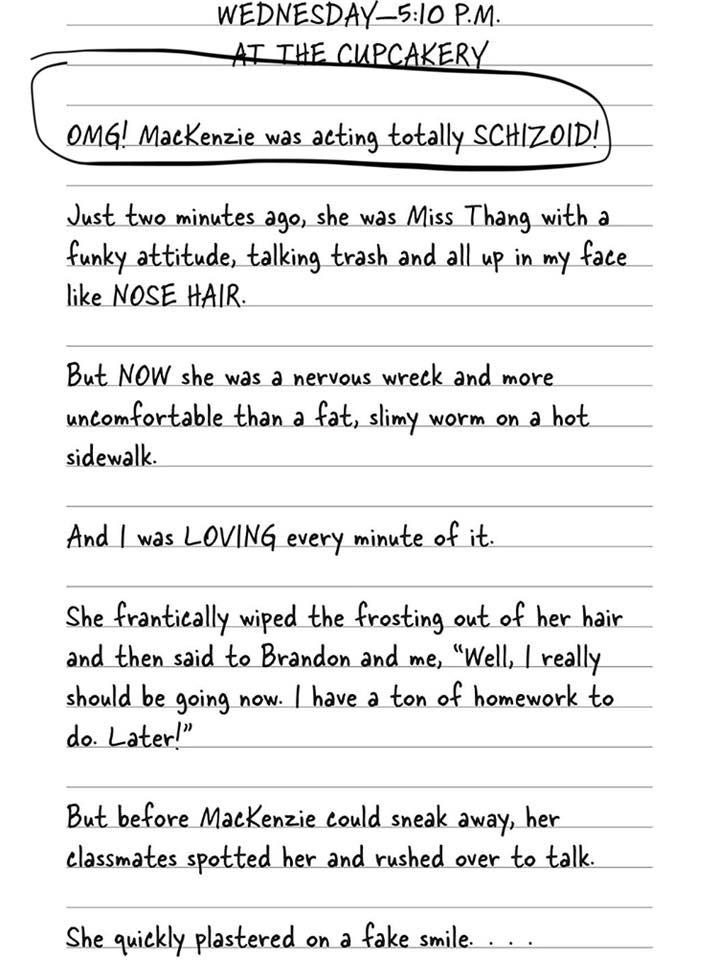
I’m talking specifically about the use of phrases such as “totally SCHIZOID!” etc. to describe the narrator’s peers. (I am also not 100% sure what the author means by “acting schizoid,” and I don’t think she does, either.)
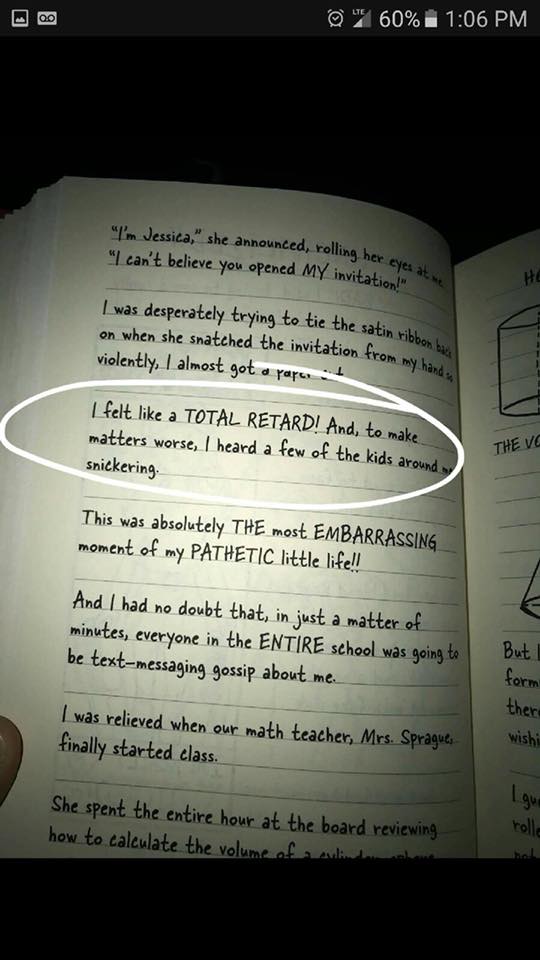
Dropping “RETARD” (please note the caps), even as a self-descriptor, is unacceptable. Come on, people. I thought we were better than this. The sad part is, the author could have gotten rid of the problematic language without negatively affecting the rest of the content. Cutting it would have actually made the book better. I’m wondering where the editor was in this process, if there even was one. I’m wondering why we still live in a world where this kind of thing manages to slip by largely uncontested.
Where did the narrator (a 14-year-old girl) learn this language? Why does she think it’s okay to casually throw around such hateful, derogatory terms? Why isn’t this addressed in the book? And more importantly, why did the author think it was okay to write this in a children’s book without any sort of disclaimer?
Kids don’t come up with “you’re trash because X/Y/Z” on their own. They hear it from somewhere else, accompanied by the implication that it’s acceptable to dehumanize others for being different and perpetuate that toxicity ad infinitum. And this is a powerful reminder that none of us exist in a vacuum.
We can’t bubble-wrap our children, nor should we. There will always be bullies. There will always be stigma. But what we can do–what we must do–is educate ourselves and our children about the glorious range of people who share this planet with us. We must teach them accountability and respect. We must teach them that they are okay just the way they are and that the limitless expanse of diversity makes the world a far more beautiful, interesting, and magical place to live.
I am not in favor of censorship. What I am in favor of is self-awareness and recognizing when you’re about to fly off the rails and discriminate against an entire group of people in one broad stroke. Anyone who steps into the public eye has a duty to ensure that they are not causing harm to others. Context is also important. While this type of language would be a bit unsettling in a book written for adults (though I would take less issue with it given the audience and their assumed level of maturity and awareness), it is absolutely disturbing when it appears in a book written for children.
As a writer, an advocate, and a budding therapist, this sickens me. It’s lazy writing designed for shock value, to laugh at and “other” people who are living with mental illnesses and disabilities. Rachel Renée Russell’s writing is irresponsible at best, though I would go so far as to describe it as dangerous because these attitudes are dangerous. These attitudes have gotten people killed.
The one silver lining I can see is that a parent could pre-read the book, then use it as a jumping-off point for a discussion with their child (or children) about why such language is hurtful and not okay to use when describing another living, breathing, thinking, feeling human being.
Here’s an easy way to tell if you’re about to say something awful about another person. Take whatever adjective you were going to use–let’s say “schizoid,” for the sake of continuity–and replace that word with a group that has been historically discriminated against (but that society has collectively acknowledged was abused, stigmatized, and worse).
For example, the above passage would read “OMG! MacKenzie was acting totally JEWISH.” [Or “Black.” Or literally any other group that, when used as an adjective in a negative context, would make you look like a terrible person.]
That sounds bad, right? Does it make you feel really gross? It should. We may think we’ve conquered racism, sexism, anti-Semitism, all the other -isms…but we haven’t. We’ve barely even addressed them. All we’ve done is move on to another scapegoat, another bogeyman, another substitute that is slightly more socially acceptable but still conveys the level of disdain as older, more taboo slurs and epithets.
And what about the kids reading it who happen to have any of the conditions Russell has singled out in her books as targets of derision and malice? What happens when a child who has some form of mental illness or disability? How is a parent supposed to help heal the damage done when the hatred is right there in black and white for the child to see? The message sent by these books is that it’s acceptable to make people feel less-than because of something they cannot control.
And readers, you should never let anyone make you feel like less than you are, period. You are beautiful. Your brain is beautiful. You are strong. And we all deserve better than this.
There are so many words in the English language relating to innocence and vulnerability, and most of them can bring me way down if I’m not careful. They provoke some ancient anxiety that I’ve come to realize, with the help of my excellent therapist, are linked to what she calls my “wounded younger self.” (I was incredibly skeptical of inner child work at first, but it is incredibly effective and incredibly healing.)
“Little” is an adjective that, when paired with certain words that also remind me of innocence, usually messes me up emotionally. That’s the word that got under my skin tonight.
I’ve been feeling kind of “off” the last few days. I recently blocked my mother completely on my phone–including the second number I thought she’d deleted until she used it to contact me after I blocked the first number–and was treated to some really unsettling dreams on Monday and Tuesday night.
Monday’s main feature involved me skipping my grandmother’s birthday party because my mother was going to be there and I knew she’d be drunk. Tuesday’s late-night horror show involved a healthy helping of guilt because I was hiding from her (in a Target, of all places) while she wailed and lamented that she “couldn’t believe [I] didn’t want to talk to her.”
Naturally, this put me in a pretty weird headspace today. Wednesdays are my big clinical days and I do group as well as individual client work. As such, I generally store my feelings away to deal with later and do a pretty good job of not thinking about them at all during the day because I’m 100% focused on my clients. (Side note: I adore them, and I’m bummed that I’m leaving my practicum site in a few weeks!)
On the drive home from class this evening, though, those neglected feelings reared their ugly collective heads and roared.
The anxiety and guilt were so powerful that I considered just going to bed early and sleeping it off.
Instead, I took a shower.
I focused hard on those thoughts and attempted to get a good, cathartic cry in. Nothing happened.
I turned the focus to that wounded younger self I mentioned and took the opportunity to literally hug myself while I waited for the conditioner to work its magic on my decidedly unruly hair. I decided to speak aloud because I’m home alone most days during the week and hey, I knew the cat wouldn’t judge me. (Audibly, anyway.)
I told my younger self that it’s okay. I told her I love her and that I’m sorry she felt like no one could keep her safe. I told her that I’m going to do it. This changed into me speaking to whatever hypothetical future child I’ll end up having. I promised that child to take the best care of it I can and to make sure it never feels afraid or lonely.
And I cried. Instead of stifling it or trying to be tough, I gave myself over to it completely–ugly, wracking sobs. After a while, those sobs turned into relieved laughter that I’m sure sounded like I’d finally gone completely ’round the bend.
I think there’s something to be said for having a good cry.
On Monday, I spoke to my clients in group about the concept of “ghosts”–they had all shared some intense and profound stories about their deepest wounds, their secret shames, their most painful memories. I told them that while they can haunt you, they can’t physically hurt you. You can start to let go of them.
I led them in one of my new favorite exercises, which is “HA!” breathing. Basically, you take a deep breath and push that breath out while making a “HA!” sound. I opened the group with the exercise and invited them to imagine themselves yelling at someone or letting frustration out. I demonstrated (because I am not afraid to look silly anymore), and they loved it. After the big, intense sharing session, I led them in the exercise again, this time instructing them to imagine the “HA!” on the exhale as them blowing out part of their ghosts.
I’m glad it was a hit, and I encourage you all to try it, readers. Howling into the void or, as I called it, “therapeutic yelling,” is incredibly cathartic.
Jeanette at My Life with PTSD & Bipolar: Mental Health Matters kindly nominated me for
Write a brief story about how your blog began. I’ve been running The Dissociated Press for five years now (holy cats, time flies!) and have been documenting my journey to mental health–or at least, relative stability and improved daily functioning. When I started this blog in 2013, my life was a total mess. I was in an unhappy marriage and missing a lot of work because I was freshly diagnosed with bipolar 1 and adjusting to my new medications. I ended up losing that job, which was a major low point.
There have been a lot of low points throughout my blog-writing history, but things have dramatically improved in the last couple of years. I escaped from that unhappy, unsupportive marriage, enrolled in graduate school for clinical mental health counseling at a great school, and got engaged to a lovely, wonderful man.
I still hit depressive episodes from time to time, but unlike my pre-medication, bad relationship days, I take comfort in the knowledge that my life is so much better than I ever could have imagined. I have a wonderfully supportive partner, and his family is incredibly encouraging of me sharing my journey. My classmates have expressed appreciation for my candor, and I’ve been able to help a lot of people through my disclosures.
Advice for new bloggers is something I haven’t really thought about, but my main piece of advice is to write for yourself first and foremost. TDP has evolved over time–at first, it was a place for me to get my thoughts and experiences out into the ether in hopes of finding others who were also struggling.
Also, I like to focus on and directly address my readers as a group in my posts and always try to end a post with a positive thought or insight. It prevents the blog from feeling dreary and helps promote the overall message: recovery is possible, and recovery never looks the same for everyone. Your journey matters. Your message matters. Your experiences matter.
As I’ve gotten healthier and stopped focusing so much on my illnesses (which are still a main focal point of the blog, albeit in a different way), I realized that my relatively small following was a great audience for information about the stigma surrounding mental illness.
I realized that everyone, but especially others living with my specific conditions (PTSD with depersonalization/derealization and rapid-cycling type 1 bipolar disorder) could benefit from learning about the latest news and treatment options. I’m building up quite the library of scholarly articles and studies, and if there’s enough interest, I plan to post a few quick-and-dirty rundowns of them.
Again, I can’t thank Jeanette for this nomination–it came out of nowhere and I feel very honored about the whole thing and appreciate being recognized for my work. Validation and recognition for what I’m doing always feels nice! Also, the badge image is really cute.
For Thanksgiving, we flew back to my hometown in the Midwest to visit my remaining family–my mother, the aunt who was my legal guardian when I was a child, and another aunt who lives about an hour away from said hometown but visits regularly.
As I told my therapist this afternoon, “I don’t want to say it sucked, but…it sucked.”
I don’t want to get into any of the messy details, but I realized a few things during our brief Thanksgiving trip.
The first is that my grandmother is dead, like, for real-real. My “mom” is dead. Full stop. It’s not that I was pretending otherwise, but being in her house without seeing her there drove the point home in an unexpectedly painful way, and I had to hold it together while I was there because I knew if I lost it, so would everyone else, and then it’d be this whole terrible thing that I was just not equipped to handle.
The second is that it’s not normal to spend the week up to your flight being anxious and trying to brainstorm ways to defuse any potential arguments. It’s not normal to be five minutes from landing in your hometown and freaking out because you have no idea how many fights there will be this time or how bad they’ll get.
The third is that it’s simply not healthy for me to go “home” again. My therapist agreed with this assessment–there really is nothing there for me anymore. I’m 28 and am building my own life, my own family. If anyone wants to visit me, they know where I am. There are several large airports nearby. I never turn my phone off, though I have become more selective about when I answer calls–if I’m emotionally exhausted and have nothing left to give that day, I let the call go to voicemail.
It’s not like I’m unreachable. I just don’t want to make the effort anymore. I’m tired of throwing myself out into the wilds of my family-of-origin and hoping I come back in one piece. I’m tired of having to tell them, “Hey, I flew all the way here, can we all just get along?” I’m tired of having to put a dog into the fight. I’m tired of there even being a fight.
I went back “home,” and all I got was the flu and three days of crippling anxiety and depression.
Readers, it’s okay to set boundaries. If, like me, you’ve finally hit your breaking point, please try not to feel guilty about it. You need to take care of you first. You can’t pour from an empty cup, and life is too short to spend it with people who make you miserable.